|
Reducing racial/ethnic disparities in immunization rates is a compelling public health goal. Disparities in childhood vaccination rates have not been observed in recent years for most vaccines. The objective of this blog by Keshika Vasuja is to assess vaccination by race/ethnicity in the world. Vaccines help contain the spread of diseases and reduce morbidity and mortality. For any vaccination effort to succeed, vaccine uptake must be widespread across the entire population. However, the US population is very diverse, and there are various groups with different attitudes and beliefs regarding vaccination; this leads to disparities in vaccination rates. To discuss diversity, we need to define “race” and “ethnicity.” According to the US Census, race refers to the grouping of people based upon physical characteristics and geographic roots, while ethnicity is a cultural and social construct more than a biological one. For example, a person’s race may be identified as Hispanic, but their ethnicity may be Honduran, even if they were born and raised in the US (4). Whenever a new vaccine gets approved, health officials have to tackle the difficult question of who should be first in line to receive it. Typically, health-care workers are first, and in previous outbreaks, such as the H1N1 swine flu in 2009, people whose health was most vulnerable got priority, too. With the widely anticipated COVID-19 vaccine, there’s a new factor being considered: fairness. Disparities in vaccinations lead to disease outbreaks affecting certain groups more than others. For example, during the 1989-1991 measles outbreak in the US, American Indian, non-Hispanic black, and low-income children had a 3 to 16 times greater risk for measles than non-Hispanic white children. These same groups were also at that time recognized as being under-vaccinated.2 On October 2, the National Academy of Medicine revealed its recommendations for COVID-19 vaccine distribution in an influential 237-page framework commissioned by the National Institutes of Health and the U.S. Centres for Disease Control and Prevention. The report proposes distributing a vaccine in four phases as it becomes available. The first recipients are obvious picks: health-care workers, emergency responders, people with underlying conditions, and older adults living in group settings. This mirrors similar recommendations by the World Health Organization, and it is a foundational principle for the COVAX collaboration, a global effort to improve poorer countries’ access to a vaccine, which 171 nations have pledged to join. But for the first time in history, the report also recommends that priority be given to people who score high on the CDC’s Social Vulnerability Index, which identifies factors such as poverty, lack of access to transportation, or crowded housing that are linked to poor health outcomes. The committee of virologists, epidemiologists, economists, and other health researchers who wrote the report said the goal is to rectify the pandemic’s disproportionate burden on minorities and poor people and “work toward a new commitment to promoting health equity.” The disparities are stark: Compared with white people, African Americans, Hispanics, and Native Americans are nearly three times more likely to contract the coronavirus. Blacks are twice as likely to die. “This approach allowed us to embrace a notion of equal regard for all people, and address the underpinnings of social inequity and factors that have landed African Americans, Hispanics, and Native Americans in situations and occupations in which they are less healthy,” committee member Jewel Mullen, associate dean for health equity at Dell Medical School at the University of Texas at Austin. Analysis of flu vaccination rates shows persistent gaps and racial disparities in flu vaccination among adults. Data from the Centres for Disease Control and Prevention (CDC) show that the flu vaccination rate generally has been increasing over time but remains below the target level, with lower rates of vaccination among Black and Hispanic individuals compared to White individuals. These gaps and racial disparities in vaccination are concentrated among adults. During the 2018-2019 flu season, less than four in ten Black (39%), Hispanic (37%), and AIAN (38%) adults were vaccinated compared to nearly half of White adults (49%) (Figure 1). Vaccination rates were higher among children compared to adults and the rates for children of colour were generally equal to or higher than those for White children. 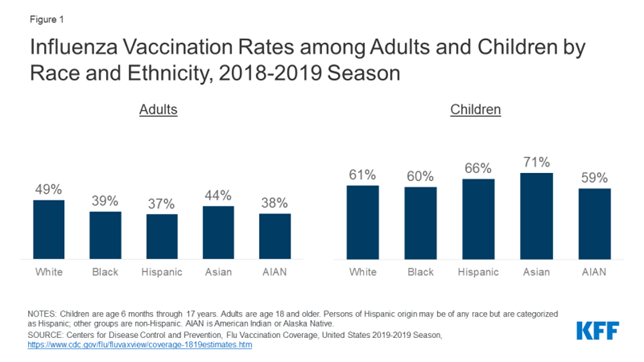 The lower vaccination rates among adults of colour, in part, reflect their higher uninsured rates. Data show that people of colour are more likely be uninsured and less likely to have a usual source of care. Seasonal flu vaccines, especially for adults, are delivered and administered primarily through a system of private distributors and providers. As a preventive service under the ACA, the vaccine is available at no charge for individuals with insurance. However, uninsured individuals either need to pay out-of-pocket for the vaccine or identify sites, such as clinics or health centres, that are offering it for free. Evidence suggests that the federally-funded Vaccines for Children (VFC) program, which provides vaccines at no cost to children who might not otherwise be vaccinated because of inability to pay, has contributed to the higher vaccination rates among children across racial and ethnic groups. However, analysis of National Health Interview Survey data illustrates the barriers to vaccination facing uninsured adults. Across racial and ethnic groups, uninsured adults were less likely to be vaccinated compared to those with private coverage across most groups.
Racial and ethnic differences in vaccination levels narrow when adjusting for socioeconomic factors analysed in this survey, but are not eliminated, suggesting that other factors that are associated with vaccination disparities are not measured by the National Health Interview Survey and could also contribute to the differences in coverage. Additional efforts, including systems changes to ensure routine assessment and recommendations for needed vaccinations among adults for all racial/ethnic groups, are essential for improving vaccine coverage. Works Cited: https://www.kff.org/policy-watch/racial-disparities-flu-vaccination-implications-covid-19-vaccination-efforts/ https://pubmed.ncbi.nlm.nih.gov/26297451/ https://www.nationalgeographic.com/science/2020/10/who-is-first-in-line-coronavirus-vaccine/ https://www.pharmacytimes.com/publications/supplementals/2017/ImmunizationSupplementJune2017/immunizations-and-health-disparities-immunizations-provided-across-a-diverse-population
0 Comments
Leave a Reply. |
Welcome to our blog, Medquity!Here we will post extra articles on health disparities to display the profound health inequities in our healthcare system. These are updated every other weekend, so check back regularly! Archives
July 2021
CategoriesHealthNeedsRx ©
Copyright 2021 |
 RSS Feed
RSS Feed
